In 2004, when Richard Sargent, Robert Shepard and I published “Reduced incidence of admissions for myocardial infarction associated with public smoking ban: before and after study” reporting that hospital admissions for heart attacks dropped when Helena, Montana passed its smoke-free law, it was controversial. Since then, many studies have confirmed and expanded this conclusion (Institute of Medicine). Chuyue Wu and colleagues’ paper, “Comprehensive Smoke-Free Laws and Cardiovascular Disease Mortality in US Counties,” substantially adds to the evidence by showing that smoke-free laws quickly reduce cardiovascular deaths and that this benefit persists and grows over time.
Specifically, they showed that in counties that implemented comprehensive smoke-free laws (workplaces, restaurants and bars) the death rate from cardiovascular disease (CVD) fell by an average of -12.0 (95%CI, -21.3 to -2.7) deaths per 100 000 population per year in the 12 years following implementation of the law. Reductions in the death rate emerged by postpolicy year 2 (-11.0; 95% CI, -21.6 to -0.3) and grew over time, reaching -25.3 (95%CI, -52.6 to 2.0) deaths avoided in year 12.
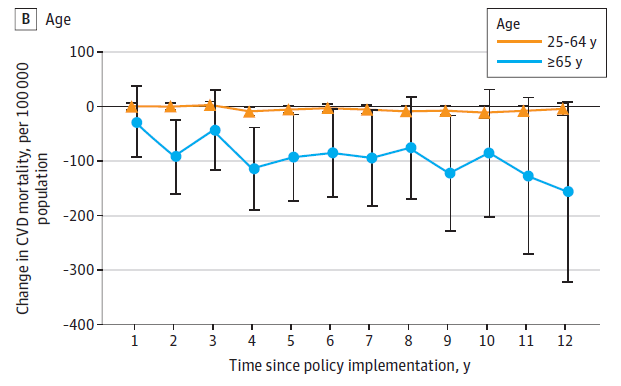
Not surprisingly, they found the biggest effects among people 65 and older (graph above): “Among adults aged 25 to 64 years, reductions were small (12-year averaged [CVD deaths per year per 100 000 population] -3.7; 95%CI, -8.0 to 0.7). In contrast, adults aged 65 years and older experienced larger reductions (12-year averaged [CVD deaths] -84.4; 95%CI, -146.0 to -22.7), with the largest reduction observed at year 12 (-155.7; 95%CI, -321.7 to 10.3). As they explained, “The larger association observed among adults aged 65 years and older may reflect higher baseline cardiovascular risk and greater susceptibility to tobacco smoke exposure. Older adults have a higher prevalence of CVD, and related comorbidities, which may increase vulnerability to both active smoking and SHS. Even short-term exposure can trigger adverse cardiovascular events making reductions in tobacco exposure more impactful in this group [citations deleted].”
They did the study by comparing CVD death rates in 38 counties with comprehensive county smoke-free laws with 103 counties with no county restrictions over time, accounting for how long the laws had been in force and controlling for median age, proportions of residents who were male, not non-Hispanic White, not currently married among individuals aged 15 years or older, without a high school diploma among those aged 25 years or older, living below the federal poverty level, working outside their county of residence, and unemployed among individuals aged 16 years or older in the labor force. All these adjustments made little difference in the results: The unadjusted reductions in annual deaths was -12.0 (-21.3 to -2.7) compared to -12.6 (-22.0 to -3.2) after adjustments. The fact that these estimates are so similar adds to the evidence that the effect of the laws is an independent effect that is unlikely to be the result of some unidentified confounding variables, a popular industry excuse for ignore unfavorable results.
The confidence we can have in Wu and colleagues’ results is further increased by the fact that they did a wide range of sensitivity and other analyses that confirmed the overall conclusion that comprehensive smoke-free laws are followed by reductions in CVD deaths.
In fact, Wu and colleagues probably underestimate the benefits of comprehensive smoke-free laws because they classified counties as smoke-free or not based on the county laws, which often just apply to unincorporated areas, not cities within the counties, which may or may not be covered by their own smoke-free laws. As they explain, “Counties classified as [smoke-free] may not have been fully [smoke-free], as some county-level smoke-free laws applied only to unincorporated areas and not uniformly to incorporated cities or towns. Counties classified as controls may have had smoke-free law coverage through municipal or state-level policies that were not captured by our exposure definition. Collectively, these sources of potential nondifferential misclassification may bias the estimated associations toward the null [i.e., underestimating the true effect].”
In short, this paper adds to the evidence that comprehensive smoke-free laws have rapid positive effects on cardiovascular disease not only by reducing hospitalizations and ambulance calls, but by reducing deaths and that these benefits persist and grow over time.
Here are the key points:
Question Are comprehensive smoke-free laws associated with long-term reductions in cardiovascular disease (CVD) mortality in US counties?
Findings In this comparative effectiveness research study using the generalized synthetic control method with staggered policy adoption, comprehensive smoke-free laws were associated with a mean reduction of 12 CVD deaths per 100 000 population annually over 12 postpolicy years, with larger reductions observed among adults aged 65 years or older, male individuals, and non-Hispanic White populations.
Meaning These findings suggest that populations in areas with comprehensive smoke-free laws experience reductions in CVD mortality, although this association varied across subpopulations.
Here is the abstract:
Importance Active smoking and secondhand smoke (SHS) exposure are major cardiovascular risk factors, and comprehensive smoke-free laws are a central tobacco control strategy. Although prior studies have demonstrated short-term reductions in cardiovascular morbidity following smoke-free policies, evidence regarding their long-term association with cardiovascular disease (CVD) mortality and potential differences across demographic groups remains limited.
Objective To evaluate the long-term association between comprehensive smoke-free laws and county-level CVD mortality and assess whether these associations vary by age, sex, and race and ethnicity.
Design, Setting, and Participants Comparative effectiveness research study using longitudinal county-level panel data and the generalized synthetic control method to evaluate staggered policy adoption across 38 treated counties that adopted comprehensive 100% smoke-free laws covering workplaces, restaurants, and bars between 2007 and 2018, and 103 control counties that did not implement smoke-free laws at any level during the study period from 2000 to 2018. Data were analyzed from May to August 2025.
Exposure Implementation of comprehensive smoke-free laws.
Main Outcome and Measures Annual county-level age-adjusted CVD mortality rates per 100 000 population overall and stratified by age, sex, and race and ethnicity. Average treatment effects on the treated (ATTs) were estimated with 95% CIs using parametric bootstrapping.
Results This study included 38 treated and 103 control counties. Prepolicy mean (SD) of county-level median age was 37.5 (3.5) for treated counties vs 39.1 (5.6) years for control counties. In treated counties vs control counties, 49.3% vs 49.5% of residents were male, and 15.3% vs 20.3% were not non-Hispanic White, respectively. Implementation of comprehensive smoke-free laws was associated with a mean annual reduction of 12.0 (95% CI, −21.3 to −2.7) CVD deaths per 100 000 population over 12 postpolicy years. Larger reductions were observed among adults aged 65 years or older, male individuals, and non-Hispanic White populations, whereas the associations among younger adults, female individuals, and non-Hispanic Black populations were smaller and less precise.
Conclusions and Relevance In this comparative effectiveness research study of county-level smoke-free laws, comprehensive smoke-free laws were associated with sustained reductions in CVD mortality. However, the magnitude of the associations varied across demographic groups, suggesting that additional strategies addressing disparities in tobacco exposure may be needed to achieve improvement in cardiovascular outcomes across all subpopulations.
The full citation is: Wu C, Habib M, Wong ND, Kuo T, Nianogo RA. Comprehensive Smoke-Free Laws and Cardiovascular Disease Mortality in US Counties. JAMA Netw Open. 2026 Jun 1;9(6):e2621170. doi: 10.1001/jamanetworkopen.2026.21170. PMID: 42340981; PMCID: PMC13294779. It is available here.
