
E-cigarette advocates Michael Pesko, Michael Cummings, Clifford Douglas, Jonathan Foulds, Thomas Miller, Nancy Rigotti, and Kenneth E. Warner recently published an editorial “United States public health officials need to correct e-cigarette health misinformation” criticizing the CDC for promoting what they claim is misinformation on e-cigarettes at the same time CDC was highlighting the dangers of health misinformation.
They “focus upon two specific examples that continue to be propagated by the US public health officials, despite evolving scientific data contradicting these assertions,” EVALI and the gateway effects of e-cigarettes.
EVALI
They criticize CDC for continuing to use the term EVALI — E-cigarette and Vaping product use Associated Lung Injury — for the suddenly recognized serious acute lung disease observed in mostly young people among e-cigarette users. They argue that it is now well-established that Vitamin E acetate, which is used as a solvent in some cannabis e-cigarettes, has been definitively demonstrated to cause EVALI and Vitamin E acetate is not used in nicotine e-cigarettes. They even cite a petition by “75 experts” asking CDC to remove “e-cigarettes” from the term EVALI. In their editorial they didn’t mention that they organized the petition or that most of the signatories were economists and that none of the signatories were pulmonologists.
In response to the petition, CDC explains (with citations to the literature) that 14% of EVALI cases were in people exclusively using nicotine e-cigarettes.
Pesko and collaborators go on to dismiss this finding, saying, “However, this ignores the reality that THC is illegal in many jurisdictions and so self-report on its use is unreliable, as shown by THC or its metabolites frequently being found in samples collected from EVALI patients claiming to only use nicotine-containing products [5].” While there is doubtless some under-reporting of THC use, this statement does not accurately represent what reference 5 actually says:
State and local health departments assigned EVALI case status as confirmed for 25 patients and as probable for 26 patients. Vitamin E acetate was identified in [lung] fluid obtained from 48 of 51 case patients (94%) in 16 states but not in such fluid obtained from the healthy comparator group. … Among the case patients for whom laboratory or epidemiologic data were available, 47 of 50 (94%) had detectable tetrahydrocannabinol (THC [the active agent in cannabis]) or its metabolites in [lung] fluid or had reported vaping THC products in the 90 days before the onset of illness. Nicotine or its metabolites were detected in 30 of 47 of the case patients (64%). [emphasis added]
Pesko and collaborators simply ignore this important detail.
I asked Laura Crotty Alexander, a pulmonologist who researches e-cigarettes, if nicotine e-cigarettes could cause EVALI. Here is what she said:
There is EVALI-VEA [Vitamin E acetate], which is the acute lung injury caused by inhalation of VEA (in THC containing vapes). But there is also EVALI-nicotine, meaning lung injury caused by the vaping of nicotine containing e-cigarettes. And that the latter is due to someone’s particular susceptibility to the combination of chemicals used to create that flavor, +/- the temperature applied, +/- other exposures and genetic predisposition. EVALI-nicotine was occurring for many years prior to EVALI-VEA, and is still occurring now. Case series completed or date have found that 15-20% of patients with EVALI were sole vapers of nicotine containing e-cigarettes and did not use THC in any form.
In other words, the CDC is correct and prudent.
E-cigs as a gateway to cigarettes
Pesko and collaborators write, “The [Surgeon General]-sponsored public information website about e-cigarettes, entitled ‘Know the Risks: E-cigarettes and Young People [16]’, states that ‘e-cigarette use is associated with the use of other tobacco products’. While technically accurate, many have misinterpreted this statement to mean that nicotine vaping causes young people to smoke cigarettes.” In making this criticism they ignore two important facts.
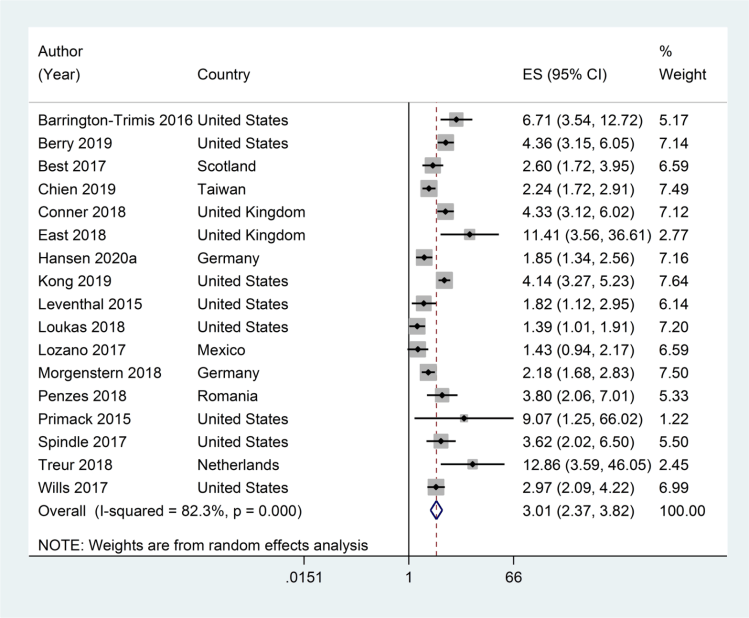
First, the longitudinal studies show that youth who initiate with e-cigarettes have about 3 times the risk of going on to smoke cigarettes compared to those who do not initiate nicotine use with e-cigarettes (meta-analysis below). Longitudinal studies are the gold standard for demonstrating causality in epidemiology.
Another meta-analysis that included cross-sectional studies and people up to 30 found even higher risks: the pooled odds ratio for progression from e-cigarettes to cigarettes was 4.6.
Second, they ignore the fact that e-cigarettes have expanded the nicotine market by attracting youth at low risk of initiating nicotine use with cigarettes.
Instead, they wave their hands and argue that if the gateway was real, youth smoking rates would be rising when, in fact, they have continued to fall. No one has ever claimed that every youth who starts with e-cigarettes would go on to cigarettes, so there is no reason to expect that smoking would increase. What the evidence actually shows, however, is that the rate of decline of smoking among youth slowed (more evidence) after e-cigarettes entered the market. That is exactly what the epidemiology predicts would happen because of the gateway.
Pesko and collaborators also ignore evidence that intensity of use and levels of addiction have increased over time among adolescent e-cigarette users.
Without mentioning these important results, Pesko and collaborators criticize the CDC by citing their own econometric papers. However these are all ecological studies, not longitudinal individual-level studies. While ecological analysis does contribute to the larger evidence base, they must be interpreted in the context of individual level studies, the much stronger design.
Causality
And, of course, they conclude talking about causality:
In the future, public health officials can reduce the risk of misinforming or confusing the public by acknowledging when evidence is incomplete or based on statistical association rather than clear evidence of causality and by updating any statements or recommendations quickly when plausibly causal or otherwise significant new evidence becomes available [24, 25]. Doing this could help to reverse the trend of declining trust in public health institutions [41] and will benefit long-term public health.
As described above, the CDC has taken care — even understated — the evidence that e-cigarettes cause disease and prolong the tobacco epidemic.
The Bottom Line
The one thing we can agree on is the Surgeon General’s statement at the beginning of Pesko and collaborators’ editorial: “Health misinformation is harmful as it can cause confusion and sow mistrust regarding the adoption of public health recommendations and policies.“
In upholding FDA’s decision to deny a marketing order for Avail e-cigarettes, federal Judge J. Harvie Wilkinson wrote that Avail “encourages us to neglect the forest for the trees” by focusing on procedural objections rather than the FDA’s mandate to protect public health. The same could be said about Pesko and collaborators’ editorial.
Indeed, the selective and misleading citation of evidence, huffing an puffing about “causality” and ignoring the forest for the trees reminds us of the tobacco industry’s longstanding techniques for arguing that smoking (and secondhand smoke) doesn’t cause disease.

How about telling us which, if any, of the authors are taking tobacco money (directly or indirectly).
LikeLike
All the authors have long histories of working to reduce cigarette use. Several have participated in suing cigarette companies. Ken Warner did support Juul’s efforts to overturn San Francisco’s e-cigarette regulations and replace them with Juul-written rules (details in https://pubmed.ncbi.nlm.nih.gov/33476232/). But I am not aware of any money changing hands (and would be surprised if that was the case).
LikeLike